What is Bladder Cancer?
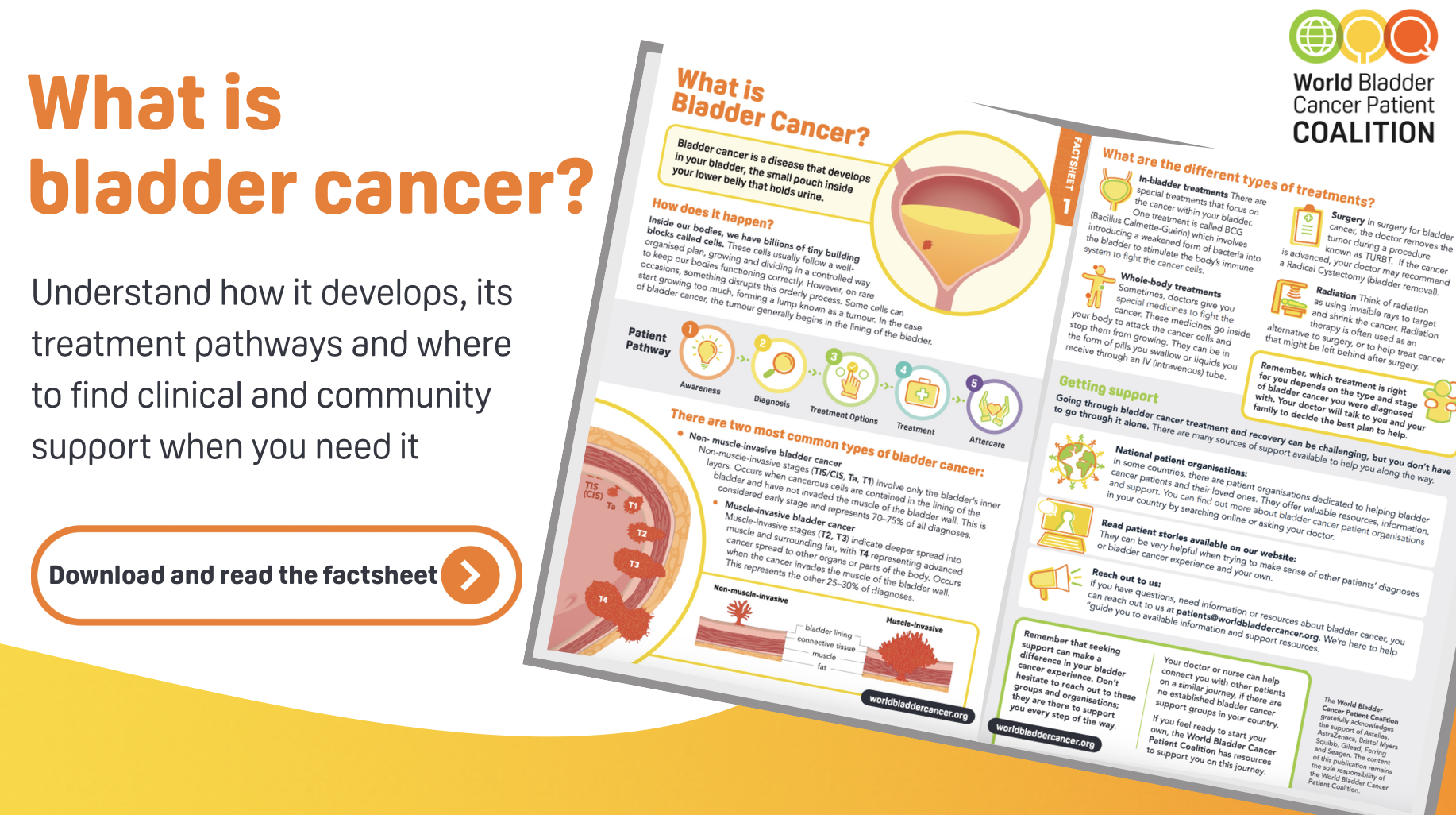
Bladder cancer is a disease that starts in the cells lining the bladder: the small, muscular pouch in your lower abdomen that stores urine before it leaves your body. It is the ninth most common cancer in the world and is diagnosed in more than 614,000 people globally every year.
Like all cancers, it begins when some of the body’s cells stop following their normal growth rules. In bladder cancer, this usually happens in the inner lining of the bladder. Some tumours stay in that lining; others grow deeper into the bladder’s muscle wall. How far the cancer has grown is one of the most important things your doctor will look at.
How does the bladder work?
To understand bladder cancer, it helps to know a little about how the urinary system works.
- The kidneys act as natural filters, removing waste from the blood and producing urine.
- The ureters are thin tubes that carry urine from the kidneys down to the bladder.
- The bladder is a stretchy, muscular pouch that expands as it fills and contracts when it is time to empty. Most bladders can hold up to about half a litre of urine.
- The urethra is the tube that carries urine out of the body.
The inside of the bladder is lined with special cells called urothelial cells (also known as transitional cells). Bladder cancer almost always begins in this lining.
What are the main types of bladder cancer?
Doctors divide bladder cancer into two main groups, depending on how far it has grown into the bladder wall. This distinction is very important because it guides treatment decisions.
Non-muscle-invasive bladder cancer (NMIBC)
The cancer is only in the inner lining of the bladder and has not grown into the muscle. This is the most common type, accounting for 70–75% of all diagnoses. It includes stages Ta, T1, and carcinoma in situ (CIS). It is often referred to as early-stage bladder cancer.
Muscle-invasive bladder cancer (MIBC)
The cancer has grown deeper into the muscle of the bladder wall, and sometimes beyond it. This bladder cancer type makes up about 25–30% of diagnoses. It is more serious and requires more intensive treatment.
What types of tumour can form in the bladder?
- Papillary tumours grow out from the bladder lining on a stalk, like tiny fingers. They tend to grow into the open space of the bladder rather than into the wall.
- Sessile tumours lie flat against the lining and are harder to detect. They are more likely to grow deeper into the wall.
- Carcinoma in situ (CIS) appears as a flat, inflamed-looking patch. It is a high-grade form of the disease, meaning it is more aggressive even though it looks subtle. Around 1 in 10 people diagnosed with bladder cancer have CIS.
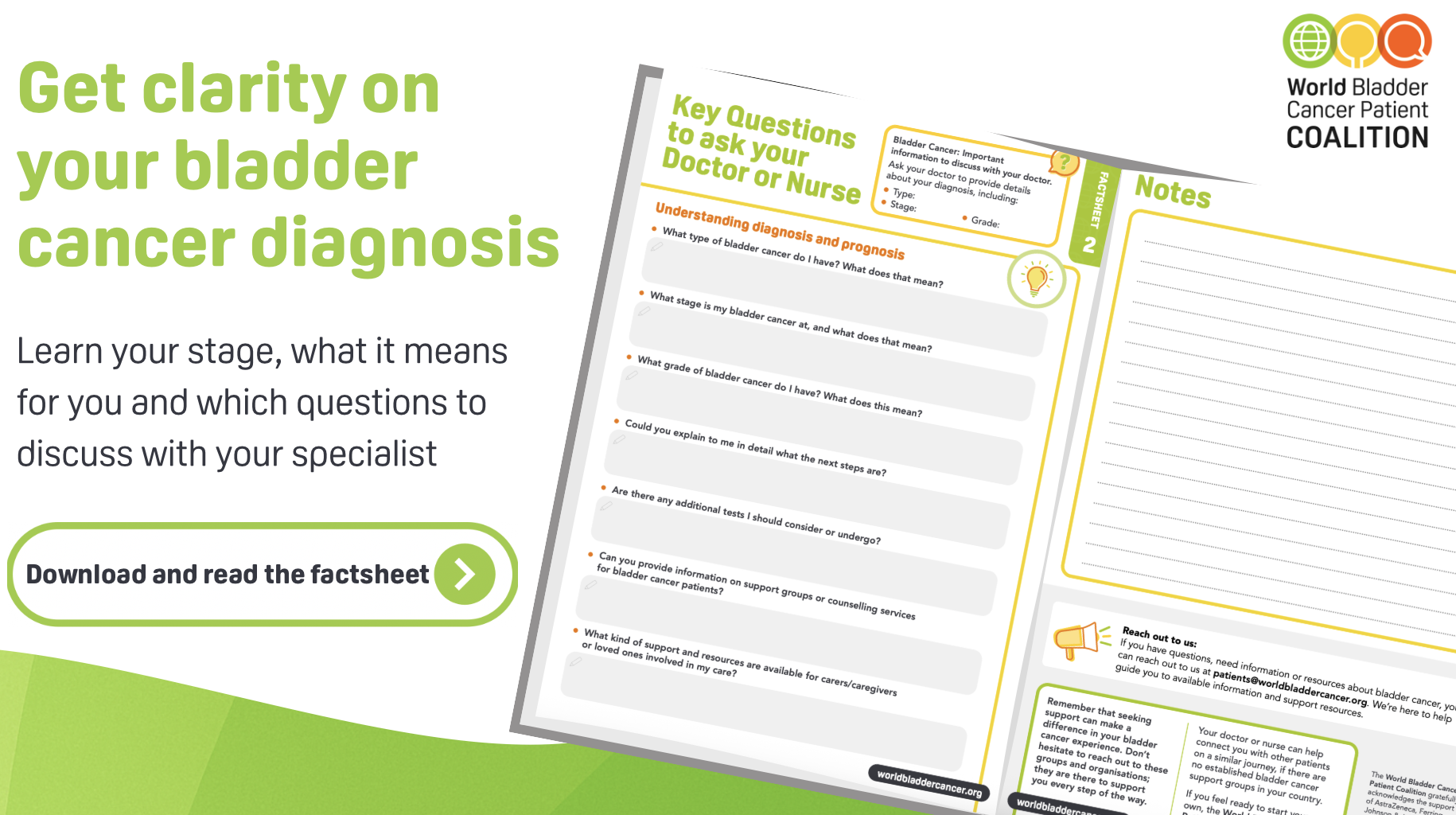
What do stage and grade mean?
After a diagnosis, your doctor will describe your cancer using two key terms: stage and grade. Understanding both will help you follow conversations about your care.
Stage: how far has the cancer grown?
- T0: No tumour detected.
- Ta: A tumour in the lining that has not grown into the bladder wall.
- TIS (CIS): A flat, high-grade tumour in the surface lining.
- T1: The tumour has grown into the connective tissue just beneath the lining.
- T2: The tumour has grown into the bladder muscle.
- T3: The tumour has gone through the bladder wall into the surrounding fat.
- T4: The tumour has spread to nearby organs, such as the prostate, uterus, or pelvic wall.
Grade: how aggressive are the cancer cells?
- Low grade: Cells look similar to normal bladder cells. They tend to grow slowly and are less likely to spread.
- High grade: Cells look very different from normal. They grow faster and are more likely to come back or spread.
Stage and grade together help your doctor choose the right treatment and predict how bladder cancer may develop.
What treatments are available?
The treatment recommended for you will depend on the type, stage and grade of bladder cancer, as well as your overall health. Your doctor will guide you through the options.
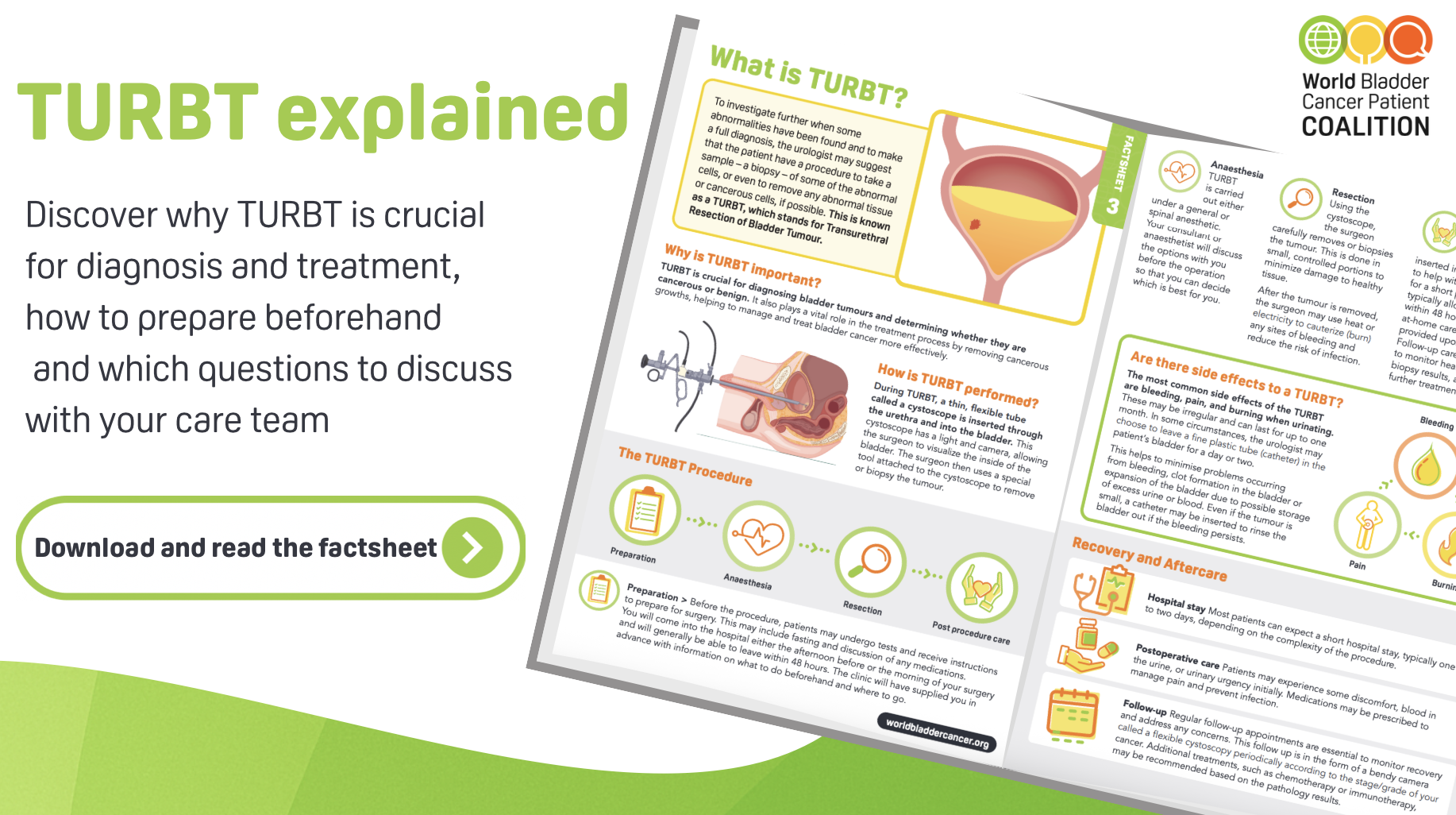
Surgery
Transurethral Resection of Bladder Tumour (TURBT) is the most common operation. A surgeon removes the tumour through the urethra without cutting into the abdomen. For more advanced cancers, the whole bladder may need to be removed (radical cystectomy), and surgeons will create a new way for urine to leave the body.
In-bladder (intravesical) treatment
For early-stage bladder cancer, medicine is sometimes placed directly into the bladder using a thin tube called a catheter. The most common is BCG (Bacillus Calmette-Guerin), which activates the immune system to attack cancer cells.
Whole-body (systemic) treatment
Chemotherapy, immunotherapy, and targeted therapy medicines travel through the bloodstream to reach cancer cells throughout the body. These may be given before surgery to shrink a tumour, after surgery to reduce the risk of it coming back, or on their own.
Radiotherapy
High-energy beams are used to kill cancer cells or shrink tumours. Radiotherapy can be used instead of surgery, or alongside other treatments to make them more effective.
Finding support
A diagnosis can feel isolating, but you are not alone. Patient organisations in many countries offer information, peer support, and a sense of community. Contact us at patients@worldbladdercancer.org and we can connect you with support in your country.
Factsheet - What is bladder cancer?
Factsheet - TURBT
Factsheet - Key questions to ask your doctor or nurse
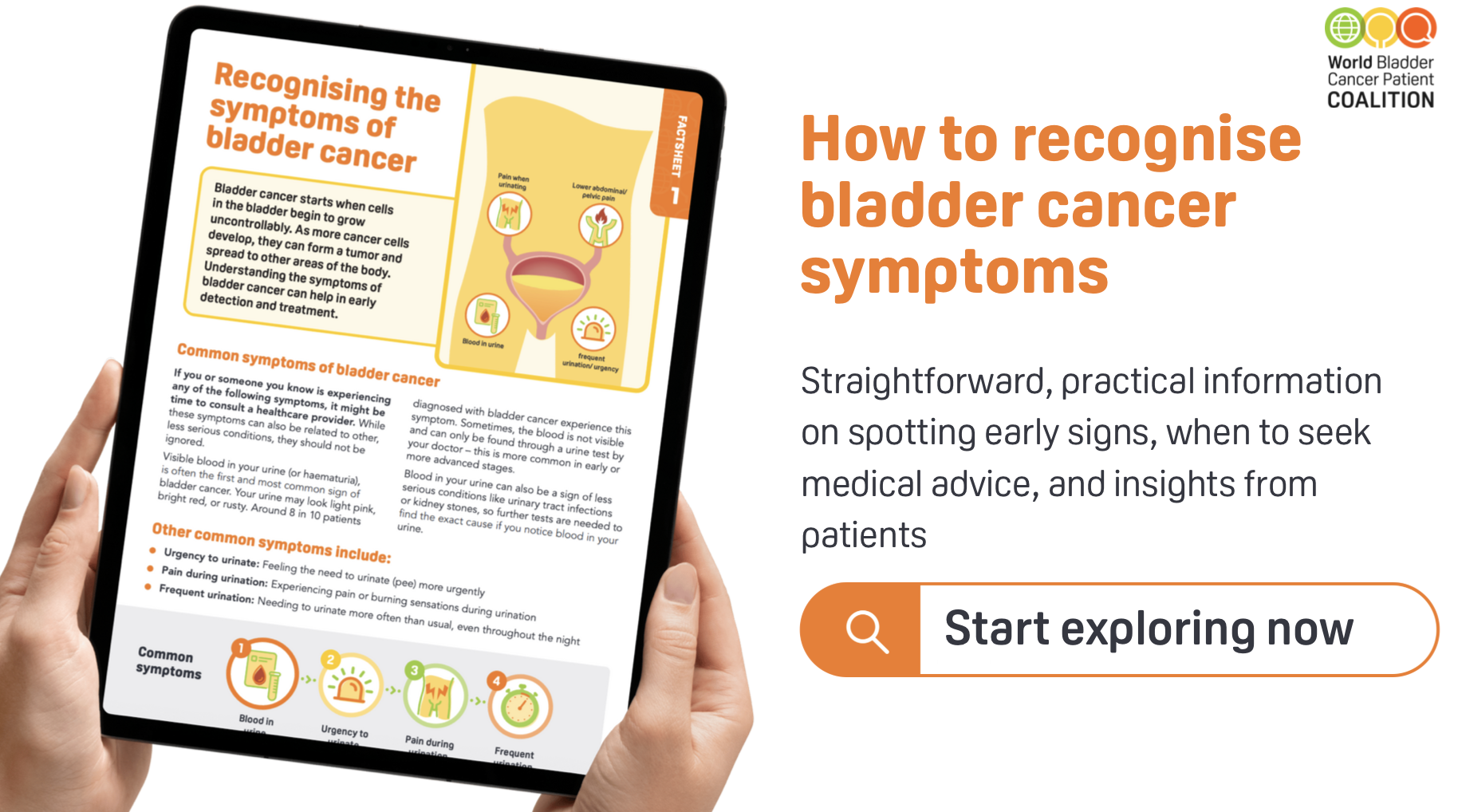
Factsheet - Recognising the symptoms of bladder cancer
Factsheet - Understand the risk factors of bladder cancer

What are bladder cancer types, stages & grades?
Bladder cancer is usually divided into two groups:
- Non-muscle-invasive bladder cancer (NMIBC): Cancer is only in the inner lining of the bladder and has not grown into the muscle. This is the most common form.
- Muscle-invasive bladder cancer (MIBC): Cancer has spread into the muscle of the bladder wall or beyond. This type is more serious and needs stronger treatments.
This difference is very important, because it guides which treatment options are recommended.
Bladder tumours don’t all look or behave the same. Doctors often describe them as:
-
Papillary tumours
Grow out from the bladder lining on a stalk, like tiny fingers or warts. They usually grow into the bladder cavity, not into the deeper wall. -
Sessile tumours
Lie flat against the bladder lining. Because they spread wider and are harder to see, they are more likely to grow deeper into the bladder wall. -
Carcinoma in situ (CIS)
A flat tumour that looks like a red, inflamed patch on the bladder lining. CIS is a high-grade form of bladder cancer, meaning it is more likely to return or spread if not treated. Around 1 in 10 people with bladder cancer are diagnosed with CIS.
es. Most bladder cancers (90–95%) begin in the bladder itself. But the same type of lining cells (urothelial cells) are also found in the kidneys and ureters.
When cancer starts there, it is called upper tract urothelial carcinoma (UTUC).
-
In the renal pelvis (the part of the kidney where urine collects).
-
Or in the ureter (the tube that carries urine from the kidney to the bladder).
UTUC is much less common, but it is treated in similar ways to bladder cancer.
Stage tells us how far the cancer has grown. It shows whether the tumour is only in the bladder lining, has grown into the muscle, or has spread outside the bladder.
-
T0: No tumour is seen.
-
Ta: A papillary tumour that has not grown into the bladder wall.
-
TIS (CIS): Carcinoma in situ, a flat high-grade tumour limited to the lining.
-
T1: Tumour has grown into the connective tissue just under the lining.
-
T2: Tumour has grown into the bladder muscle.
-
T3: Tumour has gone through the bladder wall into the surrounding fat.
-
T4: Tumour has spread to nearby organs (like the prostate, uterus, vagina, or pelvic wall).
Grade describes how abnormal the cancer cells look and how quickly they might grow.
-
Low grade (G1): Cells look more like normal bladder cells. They tend to grow slowly and are less likely to spread.
-
High grade (G3): Cells look very different from normal. They grow faster and are more likely to come back or spread.
Doctors may simply say low grade or high grade rather than using numbers.
The type of tumour shows how the cancer behaves.
The stage shows how far it has grown or spread.
The grade shows how aggressive it is.
Together, these three factors help doctors choose the best treatment and predict how the cancer might develop in the future.


